For a century, we have blamed “tired muscles” for our physical limitations. But cutting-edge science is revealing an uncomfortable truth: the muscle is merely an executor; the true drama of strength is written within the folds of the motor cortex.
By Ehab Soltan
HoyLunes — Imagine a perfectly tuned grand piano, with tempered steel strings and flawless oak wood. If the pianist sitting before it is exhausted or their hands are trembling, the music will be weak and erratic. No one would blame the piano strings. However, in traditional medicine, whenever a patient feels weakness, we have always gone straight to examining the strings: the muscle.
This metaphor reflects a profound shift in modern physiology. For a long time, muscle tissue has been considered the primary source of physical power. However, research in motor neuroscience is demonstrating that the ability to generate force depends as much on the quality of the “instrument” as it does on the precision of the electrical signal that activates it.
We are witnessing a Copernican revolution. The idea that strength is a property exclusive to tissue is dying. In its place, the Motor Brain paradigm is emerging. This shift arises from the convergence of neuroscience and neuromuscular medicine, revealing that strength is the result of constant negotiation between the brain, the spinal cord, and the muscle. In this hierarchical system, the muscle executes, but the decision regarding deployment is made within the neural networks.
The Twilight of “Muscle-Centrism”
The classic paradigm has been linear: if there is weakness, there is sarcopenia (loss of mass), fiber degeneration, or a local metabolic failure. It is the view of the body as a steam engine where only the piston matters. This mechanical model has been useful for understanding dystrophies but has relegated the role of the central nervous system as an active modulator to the background.
Today we know that, even in healthy individuals, the brain rarely allows the muscle to utilize one hundred percent of its contractile capacity. This approach leaves questions unanswered: Why are some patients with enviable muscle mass unable to generate functional strength? Why does fatigue appear long before glycogen is depleted? The answer does not lie in the “muscle-muscle,” but in the signal that awakens it. The key question is no longer “how strong is the muscle?” but “how efficiently does the brain activate it?”.
The Conductor: The Hierarchy of Movement
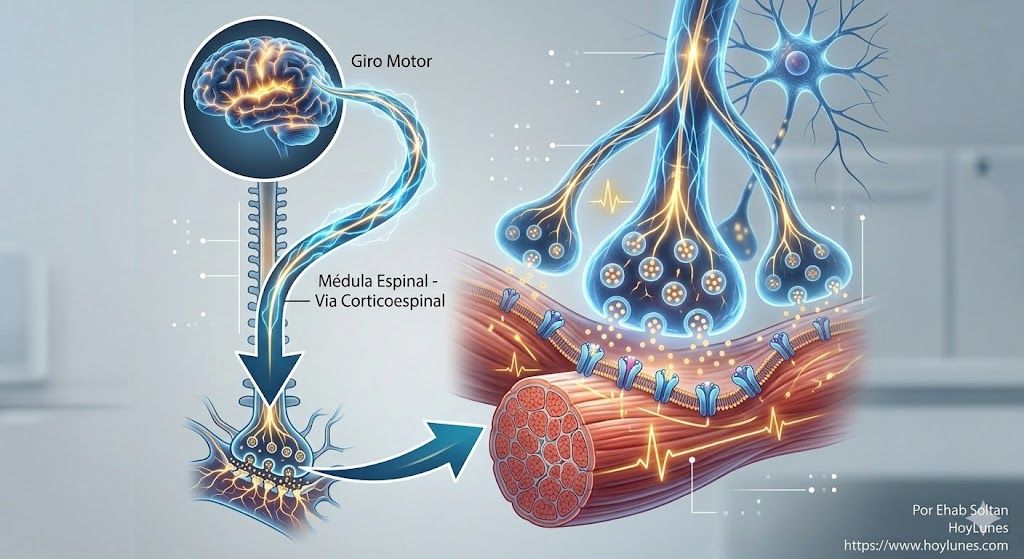
In order for you to lift a cup of coffee, “physical strength” is not required in the first instance; electrical intentionality is required. The process is a dizzying cascade:
The Spark: The motor cortex plans the gesture.
The Wiring: Upper motor neurons descend through the spinal cord.
The Relay: Lower motor neurons take over the baton.
The Execution: The muscle, finally, contracts.
From this perspective, the muscle is the final executor. If the order arrives degraded, the most powerful muscle in the world will behave like inert tissue. Each step introduces a possibility for modulation: the cortex can alter the signal intensity, and interneurons can amplify or inhibit it. Strength is the result of multiple neural decisions made in fractions of a second.
The “Fatigued Motor Brain” Hypothesis
Research at institutions such as Harvard Medical School suggests the existence of Central Fatigue. The brain acts as a “central governor”. To protect us from structural damage, the nervous system limits muscle activation preemptively. In chronic conditions—from multiple sclerosis to Parkinson’s or chronic fatigue syndrome—this regulator appears miscalibrated. The brain “decides” it must not send any more current, causing a weakness that is, in essence, neurodynamic.
This protective mechanism sometimes becomes excessively conservative, reducing activation to avoid cardiovascular or tissue damage. When this occurs, the sensation of weakness appears even when the muscle maintains its physiological capacity intact.

A New Arsenal for Diagnosis
If the problem is the signal and not the motor, our measurement tools must change. The future of medical analysis at HoyLunes points toward three pillars for directly observing the activity of the motor brain:
Transcranial Magnetic Stimulation (TMS): To measure how much energy the motor cortex is capable of firing.
Cortical Excitability Analysis: To understand if the brain is in a state of permanent “inhibition”.
Nerve Conduction Studies: To verify the integrity of the biological “fiber optics”.
Tomorrow’s Rehabilitation: Training the Mind to Move the Body
This paradigm shift transforms rehabilitation into a neuroplasticity laboratory. It is no longer enough to lift weights to hypertrophy tissue; one must retrain the brain to recruit fibers.
The brain is plastic. Even after injuries, networks can reorganize to activate the muscle in new ways. Modern therapies seek:
Neurostimulation: “Awakening” dormant areas of the motor cortex.
Motor Learning: Repetitions based on the precision of the neural signal, not just the load.
Biofeedback: Where the patient visualizes their brain activation to optimize force output.
“We are not treating shrinking fibers; we are treating disconnecting networks”.
The Muscle as a Mirror of the Brain
Exploring weakness from the motor brain perspective is not to deny the importance of exercise or nutrition. It is, simply, to stop looking at the finger when it points to the stars. Human strength emerges from an integrated system where the brain, nerves, and tissue function as a single network.
This shift in perspective expands the map. The question that 21st-century medicine must answer is: How many physical disabilities are, in reality, silences in the conversation between the brain and the body?
Sources and Authoritative References
National Institute of Neurological Disorders and Stroke (NINDS): On the hierarchy of motor control.
Journal of Neuroscience: Studies on central fatigue and inhibitory control.
The Lancet Neurology: Advances in diagnosis through cortical excitability.
Nature Publishing Group: Research on neuroplasticity applied to strength recovery.
This information is for purely informational purposes. For medical advice or a diagnosis, please consult a professional.
#Neuroscience #MotorBrain #Health #Medicine #HoyLunes #EhabSoltan