For decades, we have called almost any chronic pain in the shoulder, heel, or elbow “tendinitis”. However, modern medicine reveals that there is no inflammation, but rather a structural failure of collagen. This finding is revolutionizing sports medicine and bioengineering: from intelligent load training to biomimetic hydrogels and 3D microtendons capable of regenerating tissue without leaving scars.
By Ehab Soltan
HoyLunes – At 42 years old, Marta thought it was just fatigue. The pain in her heel appeared every morning upon getting out of bed and disappeared after walking for a few minutes. Something similar happened to Carlos, a waiter who began to notice that holding trays at the end of his shift was becoming a torment, or to Javier, a graphic designer who could no longer use his mouse without a dull discomfort in his forearm. Months later, for all of them, climbing stairs or extending an arm was already a silent negotiation with their own bodies.
Almost everyone assumes the diagnosis immediately: “I have tendinitis”. The usual home remedy consists of absolute rest, ice, and an anti-inflammatory. However, weeks pass, the pain remains, and it often worsens. Why? Because modern medical science has shown that the majority of chronic tendon problems are not inflamed.
To solve a problem, one must first understand its engineering.
The Great Confusion: Tendinitis vs. Tendinosis
The tendon is a masterpiece of biological evolution: a cord of dense connective tissue designed to transmit force from muscle to bone. Under the microscope, a healthy tendon is made up of cells called tenocytes and thousands of fibers of a protein called collagen, arranged in perfect helical chains that function exactly as micro-springs to absorb our body’s impacts.
When this structure fails due to overuse or poor loading, specialists distinguish three scenarios under the umbrella term of tendinopathy:
Tendinitis (The exception): It is an acute inflammatory response of the tendon. It occurs after direct trauma or a sudden, massive effort. It lasts just a few days or a couple of weeks.
Tendinosis (The chronic reality): There are no inflammatory cells here. What occurs is a chronic degeneration of collagen. Due to repetitive overloading, the collagen helices lose their parallelism, separate, and become disorganized. It is the equivalent of a rope that is beginning to fray and whose springs are twisting.
Tenosynovitis: Inflammation of the protective sheath surrounding the tendon (common in the hands and wrists).
“Treating chronic tendinosis with traditional anti-inflammatorios is like trying to fix a fraying rope by turning off an alarm: it blocks today’s pain, but halts tomorrow’s reconstruction”.
The dilemma of pain without inflammation: A legitimate question arises immediately: if there is no classic inflammation, why does it hurt so much? The answer from modern neurobiology is fascinating. In a desperate attempt to repair itself, the degenerated tendon abnormally develops new nerve endings and completely disorganized tiny blood vessels. These neovessels and hypersensitive nerves are responsible for amplifying the perception of pain under any physical stimulus.
The patient’s clinical error: The problem is that the term “tendinitis” continues to dominate conversations, advertisements, and quick diagnoses, even when many chronic injuries no longer respond to a classic inflammatory logic. Treating a tendinosis (frayed and lazy tissue) with traditional anti-inflammatories (such as ibuprofen) is useless in the long term. It can even delay healing, as it blocks the biological signals that the body needs to repair collagen. Popular language has become completely outdated regarding the overwhelming medical evidence of today.
A Silent Epidemic in Figures
Tendinopathies represent one of the most frequent causes of musculoskeletal pain in active adults and generate millions of medical leaves every year in Europe. The increase in sedentary work, static postures in front of screens, and repetitive movements have shifted the problem far beyond professional sports. The direct and indirect healthcare costs derived from ineffective treatments and chronic leaves represent a multi-billion dollar challenge for public health systems globally, affecting elite athletes and office workers alike.

The “Usual Suspects”: The Most Vulnerable Tendons
Although we have tendons all over our body, occupational or sporting overuse tends to concentrate on five critical points:
| Affected Tendon | Common Name of the Injury | Typical Patient Profile |
| Achilles Tendon | Achilles tendinopathy | Runners, jumpers, and weekend athletes. |
| Rotator Cuff | Shoulder impingement syndrome | Swimmers, painters, and people who work with elevated arms. |
| Patellar Tendon | “Jumper’s knee” | Basketball players, volleyball players, or CrossFit enthusiasts. |
| Lateral Epicondyle | “Tennis elbow” | Office workers (due to mouse use) and manual laborers. |
| Medial Epicondyle | “Golfer’s elbow” | Climbers, weightlifters, and users of hand tools. |
The Injury Continuum and the “Two-Week Clock”
Tendons do not break or degrade overnight; they pass through three well-defined biological phases:
Reactive tendinopathy: A rapid adaptive response to an acute overload (for example, running twice the distance all at once or typing for ten consecutive hours). The tendon thickens to try to manage the pressure. It is reversible.
Tendon disrepair: The attempt at biological repair fails if the stimulus is not stopped. The tendon matrix begins to break down at a cellular level.
Degenerative tendinopathy: The chronic phase. There are areas of the tendon where cells enter a loop of metabolic stress and the collagen is completely disorganized. The risk of rupture increases considerably here, a process that also accelerates with age as natural repair capacity declines.
This is where molecular bioengineering provides a crucial piece of data: subjecting the tendon to heavy loads immediately after an acute injury drastically worsens the microscopic twisting of the collagen. Connective tissue needs an initial protection window of approximately two weeks for those micro-springs to begin to reorganize before they can tolerate external forces. That does not mean remaining motionless in bed or resorting to total immobilization, but rather applying relative rest: strictly reducing aggressive loads and impacts while the tissue reorganizes its microscopic fibers safely.
The Modern Treatment Paradigm: Movement is Medicine
If you ask an updated specialist what to do about chronic tendon pain, their answer will no longer be “a sling and a month of absolute rest”. Prolonged rest further weakens the tendon and makes tenocytic cells even more “lazy”. Cutting-edge treatment is based on mechanotherapy (progressive loading):
Isometric Contractions (Initial Phase): Maintaining a fixed muscle tension without moving the joint (for example, standing on tiptoe on a step). They have a powerful, immediate analgesic effect on the nervous system and activate the tendon without agousing it.
Heavy Slow Resistance (HSR): Working with high loads at a very low speed. This controlled mechanical tension acts as a biological switch that forces new collagen fibers to align in parallel, restoring elasticity to the structure.
Advanced Support Terapias
When active physiotherapy needs a biological boost, sports medicine turns to tissue reactivation technologies:
Extracorporeal Shockwave Therapy (ESWT): Micro-impacts that stimulate the arrival of blood vessels to a tissue that is naturally poorly vascularized.
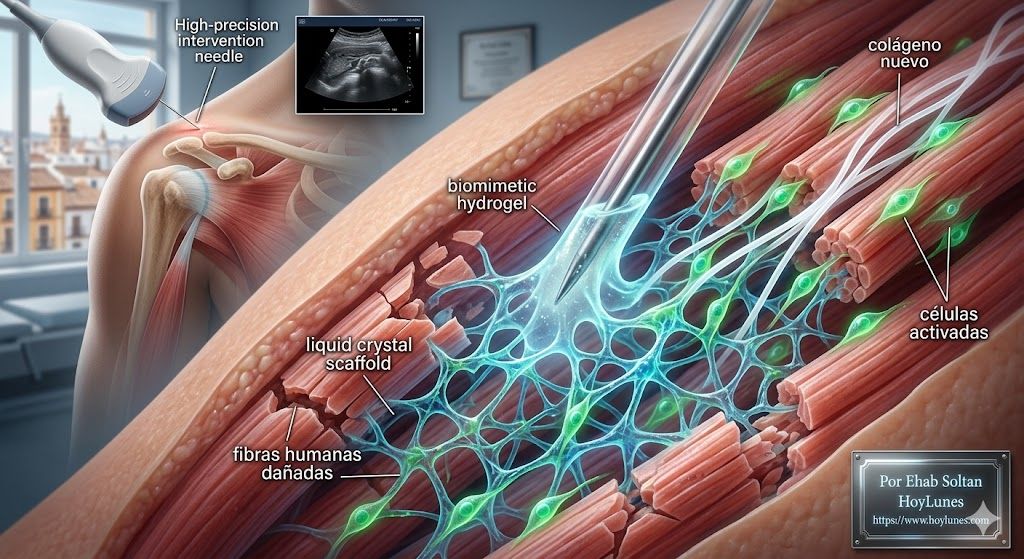
Percutaneous Electrolysis: Application of galvanic current via an ultrasound-guided needle to cause a controlled biological response that “cleans” degraded tissue.
Biological Infiltrations (such as Platelet-Rich Plasma – PRP): To accelerate cellular regeneration in selected chronic cases.
The Next Frontier: 3D Microtendons and Hydrogels
While physiotherapists apply loads in gyms, medical bioengineering laboratories are designing solutions of the future for those patients whose cells have become genetically locked in a state of chronic stress and no longer respond to exercise.
Currently, scientists are able to grow three-dimensional microtendon structures the thickness of a human hair in laboratory dishes using the patients’ own cells. These virtual environments allow testing how the tissue reacts to different mechanical and chemical stimuli.
The ultimate goal is to decipher why mammals repair injuries by creating rigid, disorganized scars, while other species of the animal kingdom, such as the zebrafish, have the astonishing ability to reactivate their cells to reconnect completely torn tendons without leaving a trace of a scar.
The most promising avenues of research point to the use of biomimetic injectable hydrogels. These gels act as a temporary scaffold within the injury, mimicking the environment of a healthy tendon to guide damaged cells and teach them how to weave collagen back into its perfect helical form. Although many of these therapies are still in preclinical or experimental phases, they represent one of the most active and exciting fields of modern regenerative medicine.

“The frustration of the modern patient collides with an uncomfortable reality: the tendon does not understand psychological urgencies or sports calendars. Its repair occurs at biological speed, not digital”.
The Collision with the Fast-Pain Industry
The frustration of the modern patient collides head-on with an uncomfortable reality: the tendon does not understand psychological urgencies, immediate work demands, or sports calendars. We live in a culture obsessed with immediacy, where pharmaceutical marketing and miracle solutions promise to extinguish any pain with a patch or a pill in a matter of hours. However, the remodeling of connective tissue is a purely mechanical and cellular process. Its repair occurs at biological speed, not digital. Forcing deadlines or masking the symptom only chronifies the degradation of collagen.
Smart Choices to Protect the Tendon
Curing a tendon is not about turning off pain with a pill, but about rebuilding its capacity to withstand the loads of daily life. The best prevention guidelines include:
Gradual loading: Muscle adapts and strengthens in days thanks to its enormous blood flow; the tendon, being a slow-metabolism tissue, needs weeks or months.
Avoid statism: Spending hours sitting or typing in the same posture generates harmful passive isometric tensions. Take short breaks and include mobility movements every hour.
Monitor morning pain: The unmistakable indicator that a tendon is suffering is stiffness when taking the first steps of the day. Ignoring it and waiting for the area to “warm up” to keep training accelerates collagen wear.
Every injured tendon is a biological rope trying to tighten again without breaking. The question that cutting-edge science and medicine ask themselves today is not just how to remove pain immediately, but how to teach the body to perfectly rebuild its invisible architecture.
Scientific Sources and References
British Journal of Sports Medicine (BJSM): Global consensus on the management of tendinopathies through mechanotherapy and progressive loading. [bjsm.bmj.com]
National Institutes of Health (NIH): Molecular bioengineering studies on collagen viscoelasticity in fatigued tendons and cellular response to early overuse. [www.nih.gov]
Harvard Medical School & Massachusetts General Hospital: Comparative research in regenerative medicine on tenocyte activation and scarless regeneration capacity in animal models (Dra. J. Galloway).
University of Michigan (Department of Orthopaedic Surgery): Development of 3D microenvironmental environments and injectable biomimetic hydrogels to reverse chronic cellular stress (Dr. A. Abraham).
Mayo Clinic & American Academy of Orthopaedic Surgeons (AAOS): Clinical guidelines for the differential diagnosis between acute tendinitis and degenerative processes (tendinosis). [www.mayoclinic.org] [www.aaos.org]
The Lancet Rheumatology: Epidemiological analysis of the socioeconomic impact, healthcare costs, and occupational prevalence of repetitive motion injuries in modern society. [https://www.thelancet.com/journals/lanrhe/home]
#Health #Medicine #PhysicalTherapy #Science #Bioengineering #Tendinopathy #ChronicPain #SportsMedicine #Rehabilitation #MedicalInnovation #HoyLunes #MusculoskeletalHealth #ScientificResearch #Wellness #Prevention #EhabSoltan